Antibiotics and the Microbiome: Effects on the Gut and Health
The infection has cleared up, the antibiotic worked—everything should actually be back to normal by now. But sometimes, after that, the body doesn’t feel like it’s back in balance: digestion goes haywire, the immune system seems to react more sensitively, or even mental well-being feels strained. This is exactly where the interaction between antibiotics and the microbiome becomes important: Can a course of antibiotics alter our microbial balance—and what consequences might that have?
Antibiotics can save lives in emergencies because they make bacterial infections treatable—infections that could become life-threatening without treatment. But this very effect also has a downside: Antibiotics do not distinguish between dangerous pathogens and the bacteria that, as part of our microbiome, perform important functions for our health. So what happens when antibiotic treatment not only fights the infection but also alters our microbial balance? How do antibiotics and the microbiome interact? Sometimes the consequences are immediately apparent. Sometimes they leave behind subtle traces—and only become apparent many years later: in the gut, the immune system, metabolism, or even the mind.
It’s easy to see antibiotics as medical miracle cures. But how do they actually work?
How do antibiotics work?
The short answer is: against bacteria. This distinction is important because it explains why we sometimes drag ourselves to the doctor when we’re completely wiped out and still don’t get prescribed antibiotics. In those cases, it’s usually a viral infection. Antibiotics are ineffective against viral infections.
A distinction is made between broad-spectrum and narrow-spectrum antibiotics. Broad-spectrum antibiotics are effective against many different types of bacteria. They are often used when the exact pathogen is not yet known or when quick action is required. Narrow-spectrum antibiotics target specific groups of bacteria and are primarily considered when the pathogen can be more precisely identified.
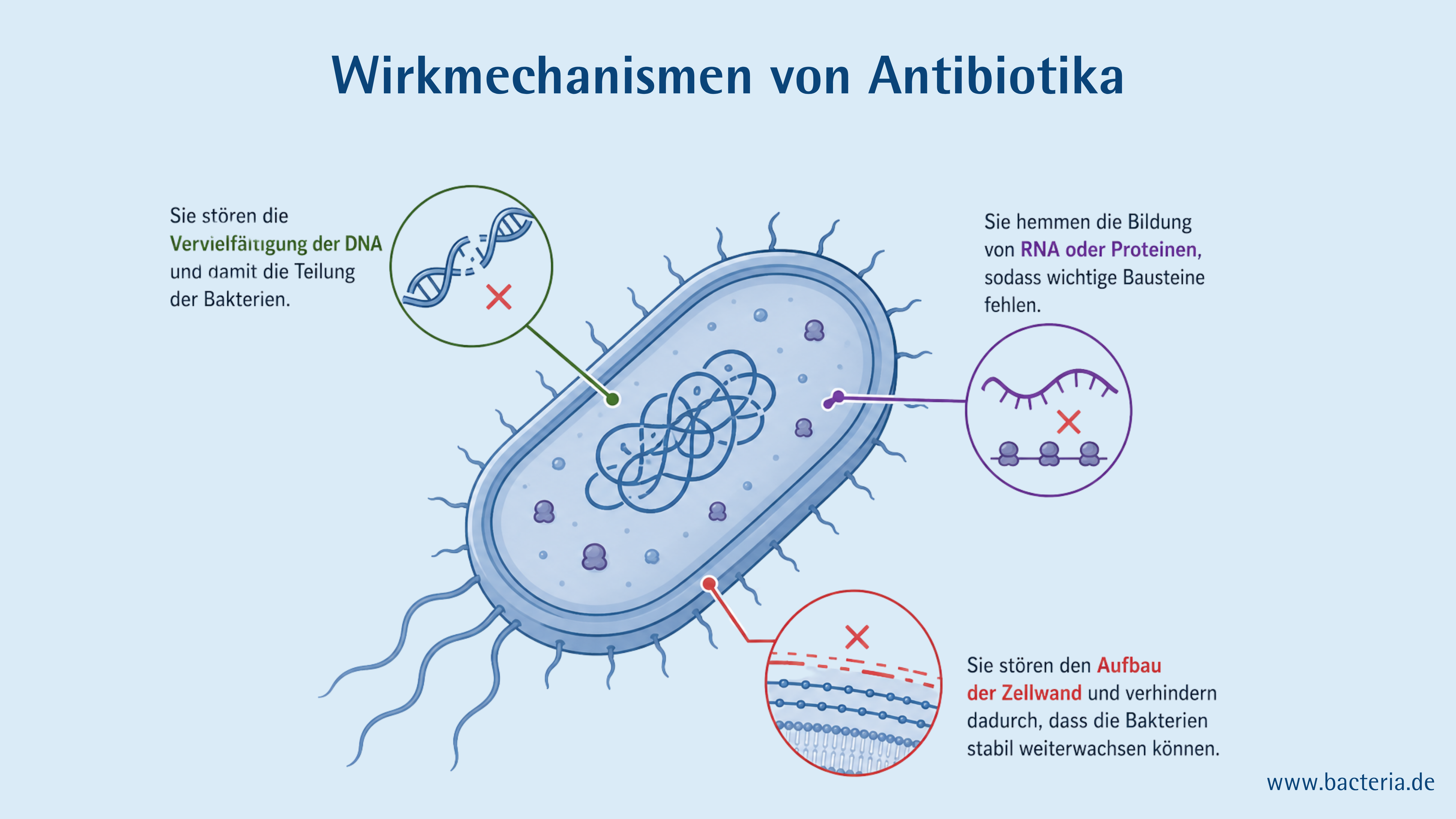
The mechanisms of action of antibiotics can generally be divided into two groups: bactericidal (bacteria-killing) and bacteriostatic (bacteria-growth-inhibiting) antibiotics. Depending on the active ingredient, they target different structures or processes that are specific to bacterial cells. This allows bacteria to be specifically targeted, while human cells are hardly affected:
- They interfere with DNA replication and, consequently, with bacterial division.
- They inhibit the formation of RNA or proteins, resulting in a lack of important building blocks.
- They disrupt the formation of the cell wall, thereby preventing the bacteria from continuing to grow steadily.
In short: Antibiotics interfere with the vital mechanisms of bacteria! This makes them an effective weapon against bacterial pathogens—but does their effect end there, or do they also have consequences that we may have overlooked for too long?
When Antibiotics Affect the Microbiome
For a long time, research into the intensive use of antibiotics focused primarily on one problem: the rise in resistance genes. In recent decades, however, another concern has become increasingly pressing—one that could have insidious and, until now, overlooked consequences for us humans: the question of what antibiotics do to our microbiome. This is because antibiotics do not act solely against pathogens. Since they attack fundamental bacterial structures, they often also affect the bacteria that perform important functions in our bodies.
Our microbiome is the totality of all microorganisms living in and on our bodies, along with their genetic information. It comprises approximately 38 trillion bacteria, over 95% of which are found in the large intestine. For a long time, the microbiome was primarily thought to play a role in digestion. Today, however, it is clear that this view vastly underestimated the importance of our microbiome. The bacteria are in constant interaction with our body: They help keep pathogens at bay, support the stability of the intestinal barrier, influence our immune system, and produce metabolic byproducts that are relevant to both our physical and mental health. If this delicate balance is disrupted, it can therefore have far-reaching consequences .
Antibiotics disrupt this balance—even in the long term. A very recent study from 2026 examined the gut microbiome of nearly 15,000 people and showed that the bacterial composition can remain altered even years after antibiotic treatment, with microbial diversity sometimes being lower as a result. Other studies also suggest that certain bacterial species do not always fully recover after antibiotic treatment and can, in a sense, leave “scars” in the microbiome.
But what impact do these changes actually have on our health?
Consequences of Antibiotic-Associated Dysbiosis
If the composition of our body’s own bacteria is disrupted, this can have various consequences. Some of these become apparent immediately after a course of antibiotics and have already been well documented scientifically. Others only become apparent over the long term and are therefore somewhat more difficult to quantify scientifically. Nevertheless, the evidence is piling up here, too!
Was ist eine antibiotikaassoziierte Dysbiose?
Eine antibiotikaassoziierte Dysbiose beschreibt eine Störung des mikrobiellen Gleichgewichts nach oder während einer Antibiotikatherapie. Dabei können nützliche Bakterien zurückgehen, die mikrobielle Vielfalt kann abnehmen und potenziell ungünstige Bakterien können sich leichter ausbreiten.
Antibiotics and the Microbiome: Acute Effects
The significant changes in our microbiome are particularly relevant because it plays a vital role in protecting us from opportunistic pathogens. This is especially important because few parts of our body come into contact with as many potential pathogens as our digestive tract. With every sip of water and every bite of food, microorganisms are constantly entering our bodies.
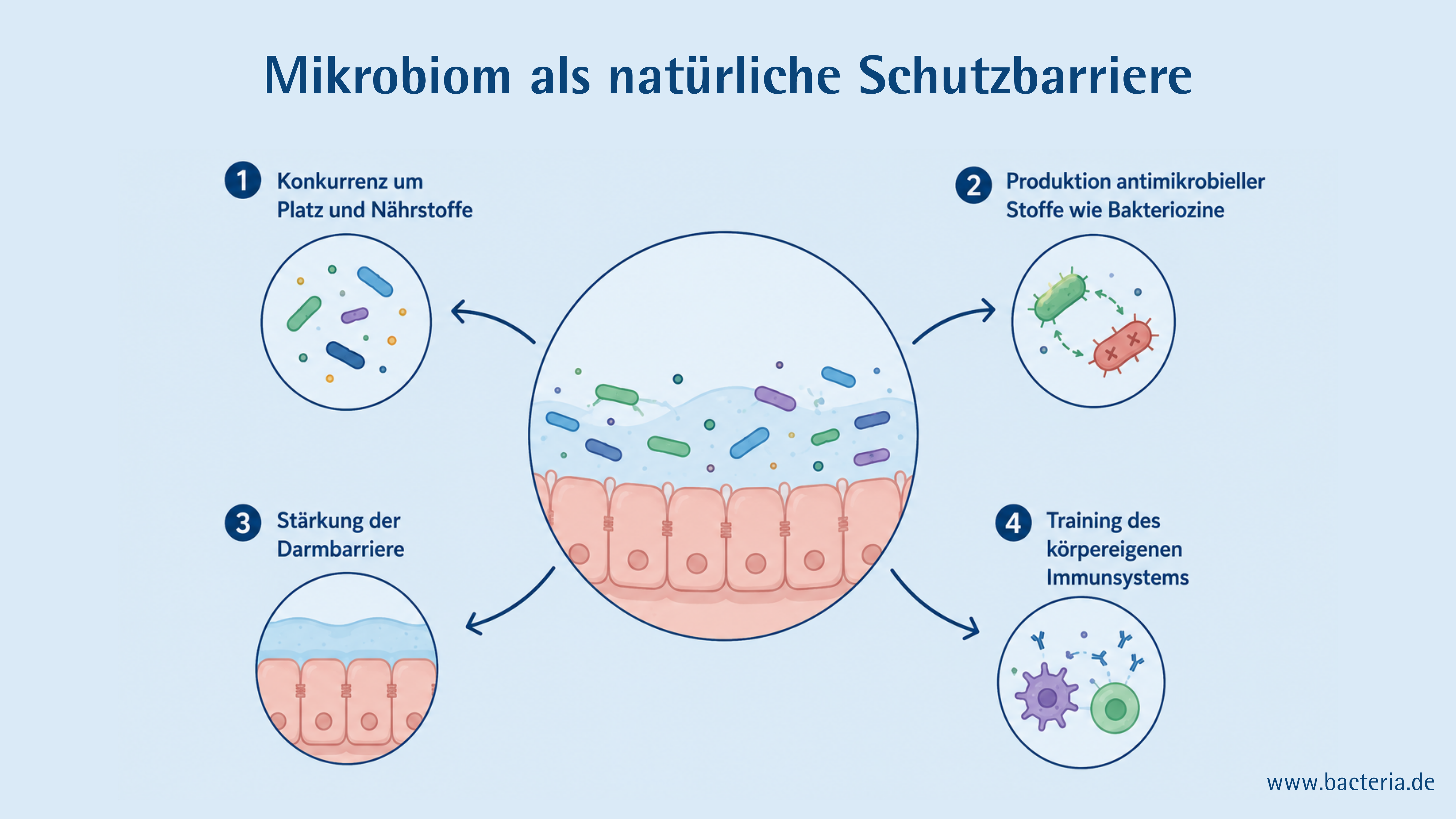
Normally, this doesn’t bother us much because our bodies are well protected . Especially in the gut, our microbiome plays a key role in this protective function—in several ways:
- Competition for Space and Nutrients
- Production of antimicrobial substances such as bacteriocins
- Strengthening the Intestinal Barrier
- Training the Body’s Own Immune System
In an instant, this defense system is thrown off balance—and pathogens can take advantage of that. The best-known of these is C. difficile, which is responsible for about 15–20% of antibiotic-associated diarrhea cases. If left untreated, an infection can become life-threatening in severe cases.
The immediate effects of antibiotic therapy are therefore not merely an abstract change in the microbiome. They can directly weaken the gut’s natural protective function and thus increase susceptibility to further health issues and infections. This is precisely why it is important to be aware of this temporary weakening and to take the body’s reactions—such as severe diarrhea, blood in the stool, or fever—particularly seriously.
Antibiotics and the Microbiome: Long-Term Consequences
1. Effects on the Intestines
More than 95% of our bacteria are found in our intestines—more specifically, in our large intestine. It is therefore not surprising that antibiotic treatment can lead to intestinal disorders.
Each year, approximately 10,000 people are newly diagnosed with inflammatory bowel disease (IBD), most commonly ulcerative colitis or Crohn’s disease. These conditions are particularly common in developed countries. The development of IBD is generally due to a combination of genetic susceptibility, environmental factors, and microbial dysbiosis, which ultimately leads to a misdirected immune response in the gut.
One of these environmental factors is antibiotic use. It is not yet fully understood how antibiotics are linked to the development of IBD. It is thought that this is because antibiotics weaken the gut microbiome, thereby triggering processes that can contribute to IBD—such as impaired nutrient absorption, a weakened mucosal barrier, altered metabolic products, and a dysregulated immune response.
Irritable bowel syndrome is a functional bowel disorder characterized by recurring symptoms such as abdominal pain, bloating, diarrhea, or constipation, with no clearly identifiable cause. Microbial dysbiosis is considered a major potential factor in the development of irritable bowel syndrome. Therefore, it is not surprising that antibiotic therapy has been linked to the subsequent development of irritable bowel syndrome. On the other hand, there are also cases of IBS—particularly IBS with diarrhea—in which symptoms can improve significantly with treatment using rifaximin, an antibiotic. This is likely due to the fact that rifaximin has a positive effect on an existing microbial imbalance and may also reduce the number of bacteria present in excessive amounts in the small intestine.
2. Effects on Metabolism
Metabolic disorders are also frequently linked to antibiotic-induced changes in the microbiome. Studies suggest that antibiotic use—particularly repeated administration during early childhood—may be associated with an increased risk of obesity later in life.
Associations have also been describedfor type 2 diabetes in large observational studies. For example, a systematic review from 2021, which included data from more than 3.9 million people, showed that antibiotic exposure was associated with an increased risk of type 2 diabetes. The effect was relatively moderate but still clearly measurable.
However, a causal relationship has not yet been conclusively proven. One proposed mechanism is that antibiotics may alter the gut microbiome, thereby reducing the production of short-chain fatty acids such as butyrate. As a result, the intestinal barrier could be weakened, allowing bacterial components such as LPS to pass more easily through the intestinal wall. This could promote low-grade inflammatory processes, which in turn could impair insulin sensitivity.
3. Effects on the Immune System
The microbiome acts as a kind of training partner for the immune system. Especially during the first years of life, the two systems develop in close tandem: The immune system learns to distinguish between harmless companions and actual invaders, and the microbiome helps it regulate its responses effectively.
When antibiotics alter this microbial training environment, the communication between the microbiome and the immune system can also be disrupted.
Studies have linked antibiotic use, particularly during the first years of life, to an increased risk of developing allergies and asthma later in life.
A link between antibiotic use and subsequent changes in the microbiome is also being discussed in the context of autoimmune diseases such asrheumatoid arthritis, multiple sclerosis, and type 1 diabetes —though the evidence from studies in this area is less conclusive so far.
Also of interest in this context is a study from 2025: It showed that newborns who received antibiotics immediately after birth later exhibited a weaker immune response to certain vaccinations. Although their immune systems did respond, the response was less robust—due to changes in the early microbiome.
4. Effects on the Mind and Brain
Through what is known as the microbiota-gut-brain axis, our gut bacteria are in constant communication with our brain.
It is therefore not surprising that mental health conditions such as depression and anxiety disorders are also linked to a dysbiotic microbiome .
A 2024 study examined nearly 200,000 people from South Korea who had taken antibiotics in the 1 to 9 years prior and found that antibiotics are associated with an increased risk of developing depression. The broader the antibiotic’s spectrum of activity—that is, the more types of bacteria it targeted—the stronger the association was.
Responsible Use of Antibiotics
Antibiotics have revolutionized medicine— and they continue to save lives to this day. Nevertheless, we must also view them with a critical eye. After all, antibiotics do not act in a vacuum. They encounter a body that is home to trillions of microorganisms. And we should keep these consequences in mind when deciding on antibiotic treatment.
The good news is: Even though antibiotics affect our microbiome, we are not completely at the mercy of these changes. Diet, lifestyle, and the responsible use of antibiotics can all play a role in strengthening the microbiome’s resilience and creating favorable conditions for its recovery.
The key message, therefore, is not to be afraid of antibiotics. Rather, it is to understand how they work—and to use them wisely.
List of Sources and Further Reading
Baldanzi, Gabriel, Anna Larsson, Sergi Sayols-Baixeras, et al. “Antibiotic Use and Gut Microbiome Composition: Links from Individual-Level Prescription Data of 14,979 Individuals.” *Nature Medicine* 32, No. 4 (2026): 1351–61. https://doi.org/10.1038/s41591-026-04284-y.
Beier, Matthew A., Soko Setoguchi, Tobias Gerhard, et al. “Early Childhood Antibiotics and Chronic Pediatric Conditions: A Retrospective Cohort Study.” The Journal of Infectious Diseases 232, no. 3 (2025): 659–68. https://doi.org/10.1093/infdis/jiaf191.
Chen, Jing, Jinlin Zhu, Wenwei Lu, et al. “Uncovering Predictive Factors and Interventions for Restoring Microecological Diversity after Antibiotic Disturbance.” Nutrients 15, No. 18 (2023): 3925. https://doi.org/10.3390/nu15183925.
Donald, Katherine, and B. Brett Finlay. “Early-Life Interactions between the Microbiota and the Immune System: Impact on Immune System Development and Atopic Disease.” *Nature Reviews Immunology* 23, no. 11 (2023): 735–48. https://doi.org/10.1038/s41577-023-00874-w.
Duan, Ruqiao, Cunzheng Zhang, Gaonan Li, Jun Li, and Liping Duan. “Antibiotic Exposure and Risk of New-Onset Inflammatory Bowel Disease: A Systematic Review and Dose-Response Meta-Analysis.” Clinical Gastroenterology and Hepatology 23, No. 1 (2025): 45–58.e15. https://doi.org/10.1016/j.cgh.2024.02.010.
Kennedy, M. S., A. Freiburger, M. Cooper, et al. “Diet Outperforms Microbial Transplant to Drive Microbiome Recovery in Mice.” *Nature* 642, No. 8068 (2025): 747–55. https://doi.org/10.1038/s41586-025-08937-9.
Kohanski, Michael A., Daniel J. Dwyer, and James J. Collins. “How Antibiotics Kill Bacteria: From Targets to Networks.” Nature Reviews Microbiology 8, no. 6 (2010): 423–35. https://doi.org/10.1038/nrmicro2333.
Krauze, Wiktoria, Nikola Busz, Weronika Pikuła, Martyna Maternowska, Piotr Prowans, and Dominika Maciejewska-Markiewicz. “Effect of Sodium Butyrate Supplementation on Type 2 Diabetes—Literature Review.” Nutrients 17, No. 11 (2025): 1753. https://doi.org/10.3390/nu17111753.
Lee, Jaewon, Sun Jae Park, Seulggie Choi, et al. “Antibiotic Exposure and Depression Incidence: A Cohort Study of the Korean Population.” *Psychiatry Research* 339 (September 2024): 115992. https://doi.org/10.1016/j.psychres.2024.115992.
Pimentel, M. “Review Article: Potential Mechanisms of Action of Rifaximin in the Management of Irritable Bowel Syndrome with Diarrhea.” *Alimentary Pharmacology & Therapeutics* 43, No. S1 (2016): 37–49. https://doi.org/10.1111/apt.13437.
Principi, Nicola, Rita Cozzali, Edoardo Farinelli, Andrea Brusaferro, and Susanna Esposito. “Gut Dysbiosis and Irritable Bowel Syndrome: The Potential Role of Probiotics.” Journal of Infection 76, no. 2 (2018): 111–20. https://doi.org/10.1016/j.jinf.2017.12.013.
Ram, Sharan, Marine Corbin, Andrea ’T Mannetje, Jeroen Douwes, Amanda Kvalsvig, and Amanda Eng. “Antibiotic Exposure in Early Life and Risk of Type 1 Diabetes: A Meta-Analysis.” Diabetes, Obesity and Metabolism 28, No. 6 (2026): 4653–70. https://doi.org/10.1111/dom.70636.
Rasmussen, Sara H., Sarita Shrestha, Lise G. Bjerregaard, et al. “Antibiotic Exposure in Early Life and Childhood Overweight and Obesity: A Systematic Review and Meta-analysis.” *Diabetes, Obesity and Metabolism* 20, no. 6 (2018): 1508–14. https://doi.org/10.1111/dom.13230.
Reynolds, Hayley M., and Matthew L. Bettini. “Early-Life Microbiota-Immune Homeostasis.” Frontiers in Immunology 14 (October 2023): 1266876. https://doi.org/10.3389/fimmu.2023.1266876.
Ryan, Feargal J., Michelle Clarke, Miriam A. Lynn, et al. “Bifidobacteria Support Optimal Infant Vaccine Responses.” *Nature* 641, no. 8062 (2025): 456–64. https://doi.org/10.1038/s41586-025-08796-4.
Salamatullah, Hassan K., Lamar AboAljadiel, Mumen H. Halabi, et al. “The Association between Antimicrobial Exposure and Subsequent Multiple Sclerosis Risk: A Systematic Review and Meta-Analysis.” *Multiple Sclerosis and Related Disorders* 107 (March 2026): 106936. https://doi.org/10.1016/j.msard.2025.106936.
Sultan, Alyshah Abdul, Christian Mallen, Sara Muller, et al. “Antibiotic Use and the Risk of Rheumatoid Arthritis: A Population-Based Case-Control Study.” BMC Medicine 17, No. 1 (2019): 154. https://doi.org/10.1186/s12916-019-1394-6.
Zhou, Jielin, Yan Lin, Yong Liu, and Keyang Chen. “Antibiotic Exposure and Risk of Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis.” Environmental Science and Pollution Research 28, No. 46 (2021): 65052–61. https://doi.org/10.1007/s11356-021-16781-3.